Researchers at the University of Pittsburgh, UPMC Hillman Cancer Center and the National Cancer Institute report that combining CAR T cell immunotherapy with a targeted radiopharmaceutical significantly improved tumor regression in preclinical models of neuroblastoma, a rare and aggressive cancer that usually forms in nerve tissue outside the brain and primarily affects children. The findings were published in Cell Reports Medicine.
Compared with radiation therapy alone, the addition of CAR T increased tumor shrinkage and complete response rates by 80%, suggesting the promise of combination treatment to improve cancer outcomes in the future.
"In this study, we used CAR T cell therapies that have been tested in clinical trials at the National Cancer Institute for children with recurrent neuroblastoma," said senior author Ravi Patel, M.D., Ph.D., director of radiopharmaceutical therapy in the Department of Radiation Oncology at UPMC Hillman Cancer Center.
"However, current cellular therapy approaches have limited efficacy in solid tumors such as neuroblastoma. Our results may offer a way to improve the therapeutic effect of these CAR T cell therapies in solid tumor cancers."
CAR T cell therapy—where a patient's disease-fighting T cells are engineered to recognize and attack cancer—has transformed treatment for certain blood cancers but has shown limited success in solid tumors like neuroblastoma.
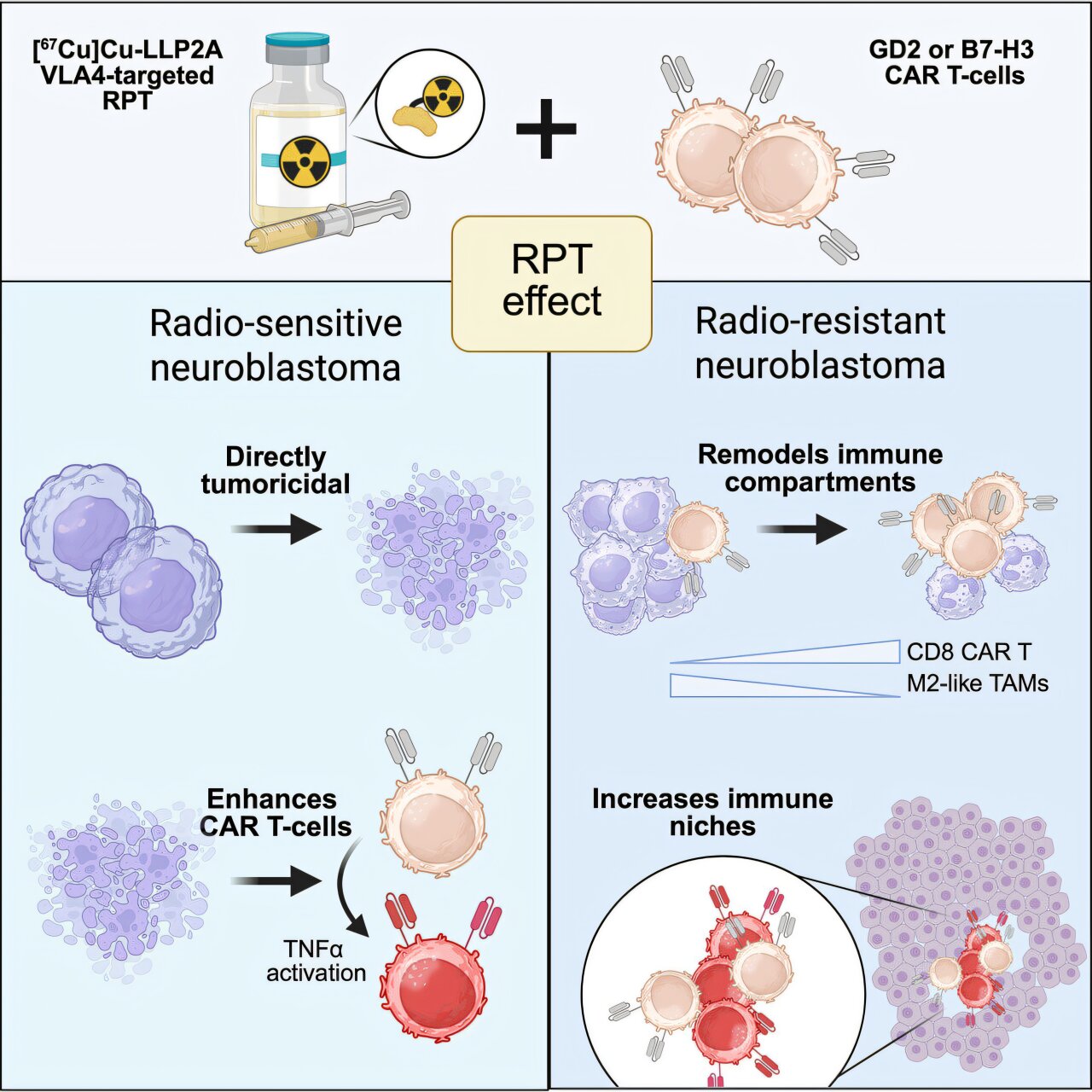
In this study, researchers paired CAR T with a systemically delivered radioactive drug, [67Cu]Cu-LLP2A, that targets a receptor expressed on tumor and immune cells called VLA-4. Once bound to its receptor target, the drug delivers localized radiation directly to the tumor and its surrounding microenvironment.
Unlike conventional radiation, which is delivered from outside the body to a fixed location, radiopharmaceuticals circulate in the bloodstream and can reach cancer cells throughout the body, including metastatic sites.
The researchers found that the combination therapy worked through different mechanisms depending on the tumor's sensitivity to radiation.
In radiation-sensitive tumors, the radiopharmaceutical directly damaged cancer cells and triggered an inflammatory response that effectively "primed" the tumor to respond better to CAR T cells.
However, in tumors resistant to radiation, the drug did not kill cancer cells directly. Instead, it reshaped the tumor microenvironment—the network of cells and molecules surrounding a tumor that can suppress immune attack—by reducing suppressive immune cells and allowing CAR T cells to enter. It converted what researchers describe as a "cold" tumor into one more open to immune attack.
The combination outperformed each treatment alone, including complete tumor regression in a substantial portion of cases.
"That's the innovation that this paper presents," added Patel. "Radiopharmaceuticals have typically been used on their own, and combinations are still being explored. Using them with CAR T cells is a new approach."
The research is preclinical, meaning it was tested in laboratory models rather than patients, and additional work is needed before it can move into human studies. Next steps include identifying biomarkers to help determine which patients are most likely to benefit, exploring how imaging could guide more precise treatment decisions, and establishing safe dosing and toxicity profiles.
The findings point to a potential new approach to one of the biggest challenges in solid tumor immunotherapy: helping CAR T cells penetrate and function within a suppressive tumor environment. If successful, this strategy could help expand CAR T beyond blood cancers and eventually offer new options for children with hard-to-treat disease.
